

Abstract
Background: Use of prophylaxis is the evidence-based strategy to prevent joint bleeds and reduce arthropathy for patients with severe hemophilia however, prophylaxis has not been universally adopted in the United States. Amongst patients with severe hemophilia enrolled in the ATHNdataset, the largest database of patients with disorders of hemostasis and thrombosis in the United States, as of 2015, 37% of patients with hemophilia A, and 45% of patients with hemophilia B do not receive prophylaxis. With the approval of extended half-life (EHL) factor products, patients and providers have options for less treatment-intense and burdensome prophylaxis. With the changing landscape of available hemophilia products, we aimed to quantify the number of patients treated at U.S. HTCs on prophylaxis utilizing the ATHNdataset with the objective determining the impact of EHL products on the proportion of patients with severe hemophilia receiving prophylaxis and to characterize use of prophylaxis according to age, race and ethnicity, geographic region, and payer.
Methods: The ATHNdataset, a HIPAA compliant limited dataset sponsored by the American Thrombosis and Hemostasis Network (ATHN), was accessed as of June 30, 2018. The proportion of subjects with severe hemophilia on prophylaxis were compared to those on demand by age cohort. The proportion of subjects on prophylaxis was analyzed by race, ethnicity, insurance status, and hemophilia treatment center region. For each group receiving prophylaxis, the product (EHL versus standard half-life (SHL)), dose and frequency of treatment was analyzed.
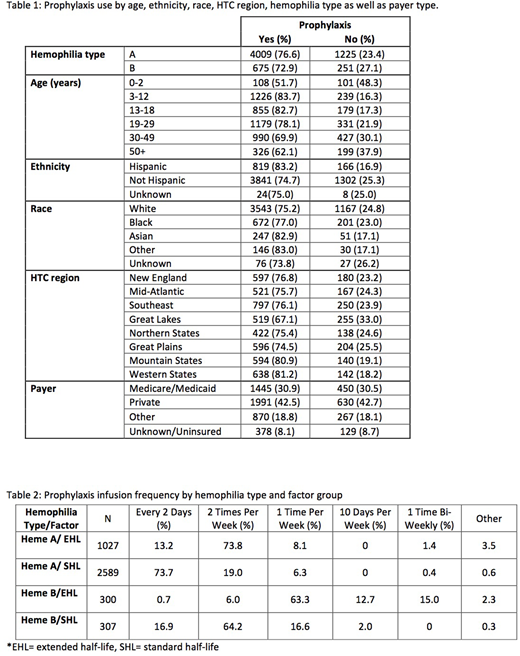
Results: ATHNdataset included 6,160 severe hemophilia patients using factor replacements, 5,234 individuals with hemophilia A and 926 individuals with hemophilia B. Overall, 76.0% (n=4,864) of patients with severe hemophilia are on prophylaxis whereas 24.0% (n=1426) are on demand; this included a total of 76.6% of patients with severe hemophilia A and 72.9% of patients with severe hemophilia B on prophylaxis. Treatment type (prophylaxis or not) had significant associations with age (p-value <0.001), ethnicity (p<0.001), race (p=0.005), hemophilia treatment center (HTC) region (p<0.001), and hemophilia type (p=0.015) (Table 1). Prophylaxis was not significantly correlated with payer (p=0.847) with a similar number of patients with Medicare/Medicaid or private insurance receiving prophylaxis.
Among patients on prophylaxis, 30.8% (n=1,462) are prescribed EHL products including 27.4% of patients with hemophilia A and 50.4% with hemophilia B. In terms of dosing frequency (n=758), 73.8% of hemophilia A patients on prophylaxis receive EHL two times per week while 73.7% (n=1,906) receive SHL every other day (Table 2). Of hemophilia B patients using EHL products, 63.3% of patients receive prophylaxis once weekly, 12.7% every 10 days, and 15.0% every 2 weeks (Table 2).
Discussion: The ATHNdataset highlights increased use of prophylaxis over the past 3 years in the U.S. with 76.6% of patients with severe hemophilia A and 72.9% of patients with severe hemophilia B currently receiving prophylactic therapy as compared to 63% and 55% of patients, respectively, in 2015. Further, the majority (83.7%) of patients are beginning prophylaxis according to the World Federation of Haemophilia recommendation to initiate prophylaxis by three years of age. There has been an uptake of the use of EHL factor products including a majority of patients (50.4%) with severe hemophilia B. Although not captured in the ATHNdataset, a plausible reason for the increased uptake of EHL in the hemophilia B population includes the data that 91% of patients are able to dose between weekly or less frequently. As the hemophilia treatment landscape continues to evolve, it is important to continue to understand the adoption of these new products into practice and to examine their real-world impact.
Malec:Shire: Consultancy; Bioverativ: Consultancy; Bayer: Consultancy; Bioverativ: Research Funding. White:Biomarin: Other: DSMB; Bioverativ: Other: DSMB; Bayer: Other: GRAC; Shire: Other: Physician Leadership Group; Novo Nordisk: Consultancy; Asklepios: Other: Scientific Advisory Board; Invitrox: Other: Scientific Advisory Board; Pfizer: Equity Ownership. Croteau:Biomarin: Consultancy; Bioveritiv: Consultancy; Catalyst Biosciences: Consultancy; CSL-Behring: Consultancy; Genetech: Consultancy, Research Funding; Novo Nordisk: Consultancy; Octapharma: Consultancy, Honoraria, Research Funding; Pfizer: Research Funding; Spark Therapeutics: Research Funding; Tremeau Pharmaceuticals: Consultancy; Bayer: Consultancy; Baxalta/Shire: Consultancy, Research Funding. Ragni:Sangamo: Research Funding; CSL Behring: Research Funding; Bioverativ: Consultancy, Research Funding; SPARK: Consultancy, Research Funding; Alnylam: Membership on an entity's Board of Directors or advisory committees, Research Funding; Biomarin: Membership on an entity's Board of Directors or advisory committees, Research Funding; Novo Nordisk: Research Funding; Shire: Research Funding; MOGAM: Membership on an entity's Board of Directors or advisory committees.

